
|
August 8, 2020 - No. 29
|


 CPC(M-L) calls on
Canadians to show solidarity with the people of Beirut and all our
compatriots here in Quebec and Canada by contributing to the
fundraising campaign initiated by the Centre National Libano Canadien
(CNLC) to assist the people of Lebanon, especially the residents of
Beirut who are hard pressed for relief after the explosion.[
CPC(M-L) calls on
Canadians to show solidarity with the people of Beirut and all our
compatriots here in Quebec and Canada by contributing to the
fundraising campaign initiated by the Centre National Libano Canadien
(CNLC) to assist the people of Lebanon, especially the residents of
Beirut who are hard pressed for relief after the explosion.[
|
|

 On July 22,
Federal Court Justice Ann Marie McDonald invalidated the section of
Canada's Immigration and Refugee Protection Act IRPA[1] and the Immigration and Refugee
Protection Regulation (IRPR)[2] that designate
the U.S. a safe third country, as she found them to be "in violation of
section 7 of the Canadian
Charter of Rights and Freedoms. (Charter)"
On July 22,
Federal Court Justice Ann Marie McDonald invalidated the section of
Canada's Immigration and Refugee Protection Act IRPA[1] and the Immigration and Refugee
Protection Regulation (IRPR)[2] that designate
the U.S. a safe third country, as she found them to be "in violation of
section 7 of the Canadian
Charter of Rights and Freedoms. (Charter)"
However, the Federal Court Justice suspended the declaration of invalidity for a period of six months, "to allow time for Parliament to respond."
In Canada, the Safe Third Country Agreement (STCA) operates by deeming most foreign nationals who arrive at a Canadian land port of entry (POE) ineligible to make a refugee claim in Canada. Section 7 of the Charter stipulates that "Everyone has the right to life, liberty and security of the person and the right not to be deprived thereof except in accordance with the principles of fundamental justice."
The Applicants' Legal Challenge
The Applicants in the case are citizens of El Salvador, Ethiopia and Syria, the Canadian Council for Refugees (CCR), Amnesty International (AI) and the Canadian Council of Churches (CCC). Their challenge was brought against the Minister of Immigration, Refugees and Citizenship and the Minister of Public Safety and Emergency Preparedness.
The Applicants challenged the validity and the constitutionality of the legislation implementing the STCA, alleging that by returning ineligible refugee claimants to the U.S., Canada exposes them to risks in the form of detention, refoulement (the forcible return of refugees or asylum seekers to a country where they are liable to be subjected to persecution), and other violations of their rights, in contravention of the 1951 Refugee Convention and the United Nations Convention Against Torture.
They also argued a "causal connection" between Canada's adherence to the STCA and the deprivation of section 7 rights and submitted that liberty and security of the person interests are engaged because of the penalization of asylum seekers by U.S. authorities. Aside from asylum seekers being deprived of liberty by detention, the applicants also noted that being detained often results in a lack of basic human dignity, lack of medical care, and lack of food. Detention also "impedes the ability to retain and instruct legal counsel and increases the risk of refoulement," they wrote.
The Respondents' Arguments
Counsel for the federal government argued that even though Section 7 of the Charter may be infringed upon, safeguards and discretionary remedies exist in the IRPA. They also pointed to the option of seeking judicial review of CBSA decisions. Additionally, they argued that the Canadian Charter of Rights and Freedoms (Charter) does not apply to U.S. law or the actions of U.S. authorities.
With regard to fundamental justice, the Ministers' legal team countered that the issue lies with U.S. authorities and policies and therefore, is outside of Canada's control. In any event, they continued, the IRPA contains protection safeguards, as discretionary remedies are available. As for removals to the U.S., they claimed that the STCA is neither overbroad, nor disproportionate in its application.
The final argument of the government was that increasing the number of claimants in Canada would negatively affect the sustainability of the refugee system in Canada.
Justice McDonald's Findings
On the Applicants' challenge that the legislation implementing the STCA is contrary to section 7 and the Charter, Justice McDonald concluded that "the actions of Canadian authorities in enforcing the STCA result in ineligible STCA claimants being imprisoned by U.S. authorities." She further determined that "imprisonment and the attendant consequences are " a violation of the rights guaranteed by section 7 of the Charter."
"Section 7 considerations are two-fold," noted Justice McDonald. First, a claimant must demonstrate that the challenged law deprives her or him of the right to life, liberty or security of the person. If so, s. 7 is engaged. Once s. 7 is engaged, the claimant must demonstrate that the deprivation is not in accordance with the principles of fundamental justice ..."
 "The principles
of fundamental justice," she continued, " are concerned with
arbitrariness, overbreadth, and gross disproportionality," ... "In
order to properly assess the s. 7 arguments it is important to
understand the process that unfolds under the STCA when a claimant
arrives at a Canadian land POE and claims refugee status."
"The principles
of fundamental justice," she continued, " are concerned with
arbitrariness, overbreadth, and gross disproportionality," ... "In
order to properly assess the s. 7 arguments it is important to
understand the process that unfolds under the STCA when a claimant
arrives at a Canadian land POE and claims refugee status."
"The issue," Justice McDonald noted, "is if the actions of Canadian officials in returning ineligible STCA claimants to U.S. authorities, where they will be imprisoned, is a sufficient causal connection so as to engage liberty and security of the person interests. The evidence is clear that the most significant harm suffered is imprisonment. Additionally, there are the related harms regarding the conditions of detention and the heightened risk of refoulement.
"Deprivations of s. 7 rights caused by actors other than our own government," she wrote, "are still subject to the guarantee of fundamental justice, as long as there is a sufficient causal connection between our government's participation and the deprivation." She went on to explain that such deprivation is one in which "Canada's participation is a necessary precondition" and "where the deprivation is an entirely foreseeable consequence of Canada's participation." The fact that "STCA returnees are imprisoned by U.S. authorities," she stated, "does not immunize the actions of Canadian officials from consideration."
The evidence presented, she wrote, "confirms that CBSA officials inform U.S. officials that STCA claimants are being returned. CBSA officials are involved in the physical handing over of claimants to U.S. officials. This conduct does not make Canada a "passive participant" and it provides a "sufficient connection [...] to the offending conduct." She concluded that such action "facilitates a process that results in detention."
In response to the federal government's claim of the existence of safeguards and remedies in the IRPA, Justice McDonald described these as "largely out of reach" and therefore "illusory."
The Federal Court Justice also remarked that there is "an important distinction between the removal cases and the facts here," pointing out that "the Applicants have not had the merits or the substance of their refugee protection claims considered in any manner in Canada, nor have they had their risks assessed." They also "did not benefit from any such consideration of their claims for protection."
 "Failed
claimants," she asserted, "are detained without regard to their
circumstances, moral blameworthiness, or their actions. They are
detained often without a release on bond and without a meaningful
process for review of their detention. While responsibility sharing may
be a worthwhile goal," she noted, "this goal must be balanced against
the impact it has on the lives of those who attempt to make refugee
claims in Canada and are returned to the U.S. in the name of
"administrative efficiency." "In my view," she said, "imprisonment
cannot be justified for the sake of, and in the name of, administrative
efficiency.
"Failed
claimants," she asserted, "are detained without regard to their
circumstances, moral blameworthiness, or their actions. They are
detained often without a release on bond and without a meaningful
process for review of their detention. While responsibility sharing may
be a worthwhile goal," she noted, "this goal must be balanced against
the impact it has on the lives of those who attempt to make refugee
claims in Canada and are returned to the U.S. in the name of
"administrative efficiency." "In my view," she said, "imprisonment
cannot be justified for the sake of, and in the name of, administrative
efficiency.
"The risks of detention and loss of security of the person, which are facilitated by the STCA, are grossly disproportional to the administrative benefits of the STCA" she found. "Responsibility sharing cannot be positively balanced against imprisonment or the deleterious effects of cruel and unusual detention conditions, solitary confinement, and the risk of refoulement."
In response to the Ministers' position that a fair detention review process is available, she responded that "suggesting that those who are imprisoned will eventually be released, is not sufficient evidence of minimal impairment."
Finally, addressing the government's argument that the sharing of responsibility had been met and that if the STCA were not operative, even greater stress would be placed on the system, Justice McDonald found: "In the past, Canada has demonstrated flexibility to adjust to fluctuations in refugee numbers in response to needs." Having found that the operation of the STCA is a violation of Section 7 Charter rights, I see no principled reason to continue to allow the provisions of the STCA to be applied to this narrow category of refugee claimants, when the evidence is that they will be imprisonied upon return to the U.S."
Notes
1. Section 101(1)(e) of the Immigration and Refugee Protection Act (IRPA) reads:
"Ineligibility
"101 (1) A claim is ineligible to be referred to the Refugee Protection Division if
"(e) the claimant came directly or indirectly to Canada from a country designated by the regulations, other than a country of their nationality or their former habitual residence"
2. Section 159.3 of the Immigration and Refugee Protection Regulations (IRPR) reads:
"Determination of Eligibility of Claim
"Designation -- United States
159.3 The United States is designated under paragraph 102(1)(a) of the Act as a country that complies with Article 33 of the Refugee Convention and Article 3 of the Convention Against Torture, and is a designated country for the purpose of the application of paragraph 101(1)(e) of the Act."
(Photos: TML, VOR, Solidarité sans frontières)

Organizations Urge Federal Government
to Immediately Stop Sending Refugee
Claimants Back to U.S.
 When on
July 23, Justice Anne Marie McDonald of the Federal Court of Canada
invalidated sections of the Immigration
and Refugee Protection Act (IRPA) and the Immigration and
Refugee Protection Regulations (IRPR) that designate the U.S. a "safe
third country," she suspended her declaration of invalidity for a
period of 6 months to give Parliament time to respond.
When on
July 23, Justice Anne Marie McDonald of the Federal Court of Canada
invalidated sections of the Immigration
and Refugee Protection Act (IRPA) and the Immigration and
Refugee Protection Regulations (IRPR) that designate the U.S. a "safe
third country," she suspended her declaration of invalidity for a
period of 6 months to give Parliament time to respond.
On July 29, the three organizations which participated as
Applicants in the federal case along with the citizens of various
countries, namely the Canadian Council for Refugees, Amnesty
International Canada and the Canadian Council of Churches sent a letter[1] to Prime Minister
Trudeau, the Deputy-Prime Minister and the concerned ministers calling
upon the federal government to:
"- immediately stop sending refugee claimants back to the United States
and suspend the STCA; and
"- refrain from pursuing an appeal of this decision."
In their letter, they note that Justice McDonald's judgement "is based on extensive and compelling concerns about the prevalence, arbitrariness, and cruel and inhumane conditions associated with immigration detention in the United States, which she finds to be an "immediate and automatic" punishment for refugee claimants denied entry into Canada under the STCA."
They also note that the Federal Court decision "provides a crucial opportunity for the government to act decisively and live up to its responsibility to bring to an end years of grave violations of the rights of refugee claimants seeking protection at official land border posts between Canada and the United States."
 Also on July 29,
the three organizations issued a public statement[2] which points out
that the decision "is based on the extensive evidence presented of
wide-ranging and very serious human rights violations associated with
immigration detention in the United States, and in particular of the
actual experiences of people returned by Canada" under the STCA.
Also on July 29,
the three organizations issued a public statement[2] which points out
that the decision "is based on the extensive evidence presented of
wide-ranging and very serious human rights violations associated with
immigration detention in the United States, and in particular of the
actual experiences of people returned by Canada" under the STCA.
Arguing that the government should immediately stop returning refugee claimants to the U.S., they further explain that"[e]very day that the rules remain in effect, more people risk being returned to face imprisonment and mistreatment."
"Similarly," they continue, "the government should refrain from launching an appeal that will further prolong and protract this intolerable situation."
"By any measure," they argue, "respect for the rights of refugee claimants in the United States at this time constitutes a human rights crisis," adding that "Canada should not continue to be complicit in these deeply troubling human rights violations for another day, let alone six months."
They also point to the fact that "if refugees are able to make claims for protection at official border posts," this will "bring an end to the crossings at Roxham Road."
"Canadians have been deeply troubled by the longstanding lack of respect for the rights of refugees and migrants in the United States, which has worsened precipitously in recent years," they further point out.
"We cannot continue to send people back to the United States knowing that they will be treated in ways that are fundamentally unjust, causing grave and lasting harm," they conclude.
Notes
1. Letter re. Federal Court Safe Third Country Agreement ruling from CCR, AI and CCC
2. Organizations call on federal government to immediately stop sending refugee claimants back to the United States.
(Photos: A. Poane, Solidarité sans frontières)
Background on Canada-U.S.
Safe Third Country Agreement
The Canada-U.S. Safe Third Country Agreement forces asylum seekers fleeing repression and persecution in the U.S. to enter Canada irregularly in order to claim refugee status. All immigration and labour laws in Canada are organized to encourage the exploitation of these and other vulnerable migrants, as well as human trafficking, all in the name of national security.
Origin of the Safe Third Country Agreement
In December 2001, two months after 9/11, the Chrétien Liberal government signed the "Smart Border Declaration and Associated 30-Point Action Plan" with the U.S. to "enhance the security of our shared border while facilitating the legitimate flow of people and goods."
The Action Plan has four pillars: the secure flow of people, the secure flow of goods, secure infrastructure, and information sharing and coordination in the enforcement of these objectives.
A report to Canada's Standing Senate Committee on Foreign Affairs entitled "Smart Border Action Plan Status Report," dated December 6, 2002 -- the day after the signing of the Canada-U.S. Safe Third Country Agreement -- includes an explanation of the situation facing refugee claimants:
" #4 Refugee/Asylum Processing
"The United States and Canada have made significant progress on a Statement of Mutual Understanding which will allow them to more effectively exchange information on immigration-related issues. The two countries are also very close to an agreement which will permit the systematic sharing of information relating to asylum seekers. This will help each country identify potential security and criminality threats and expose 'forum shoppers' who seek asylum in both systems. This exchange of information will be in accordance with the privacy laws of both countries."
" #5 Managing of Refugee/Asylum Claims
"The United States and Canada have signed a Safe Third Country Agreement that allows both countries to manage the flow of individuals seeking to access their respective asylum systems. The agreement will cover asylum claims made at land border ports of entry.
"The Agreement is bound by the principle of family re-unification in determining whether an individual would be exempted from the requirement of making a claim in the first country of arrival. The Agreement also clearly identifies that individuals making a claim in either country would not be removed to another country until a determination of that person's claim has been made.
"Both countries will now finalize the regulatory framework and standard operating procedures necessary to implement this Agreement."
Coming into Force of Safe Third
Country Agreement
Trump's Executive Orders
On January 25, 2017, U.S. President Donald Trump issued two executive orders, one concerning immigration and border security and detention and the other to remove federal funding for sanctuary cities. Sanctuary cities and counties are those that refuse to cooperate with the federal government in enforcing federal immigration laws, particularly requests to detain "undocumented" immigrants. On January 27, 2017, another executive order was issued that banned entry to any non-citizen with a passport from Iran, Iraq, Libya, Syria, Somalia, Sudan or Yemen and suspended entry of refugees to the United States. All three orders served to attack the rights of immigrants and the conception and responsibilities of citizenship. They also served to further intensify the conflicts between federal and state authorities -- all of which have their own armed police forces -- and to violate the nation-to-nation relations and principles on which the recognized international rule of law is based.
Appointment of Bill Blair as Minister of Border Security and Organized Crime Reduction
On July 28, 2018, Prime Minister Justin Trudeau announced the appointment of former Toronto Police Chief Bill Blair to the newly created position of Minister of Border Security and Organized Crime Reduction. Through sleight of hand, the Trudeau government found a way to link vulnerable migrants with border security and organized crime. By making the irregular crossing of asylum seekers through Roxham Road and anywhere else in Canada an issue of law and order, Trudeau turned those seeking asylum into a criminal category, all in the name of upholding fair treatment and rule of law, which is unconscionable. Trudeau's mandate letter to the minister reads in part: "Your goals are to ensure that our borders remain secure and to lead cross-government efforts to reduce organized crime. You will work to ensure Canada's borders are managed to promote legitimate travel and trade while keeping Canadians safe and treating everyone fairly, in accordance with our laws. You will also play a leading role in our efforts to reduce gun violence. [You] are the Minister responsible for our strategy to manage the challenge of irregular migration."[1]
Appointment of Marco Mendicino as Minister of Immigration, Refugees and Citizenship
On November 20, 2019, Prime Minister Justin Trudeau appointed Marco Mendicino Minister of Immigration, Refugees and Citizenship. One of the new Immigration Minister's roles, as outlined in his mandate letter from the Prime Minister, is to "[s]upport the Minister of Public Safety and Emergency Preparedness on irregular migration, including the new Border Enforcement Strategy and continued work with the United States to modernize the Safe Third Country Agreement."[2]
Notes
1. As Toronto Police Chief in 2010, Blair was in charge of policing the G20 Summit in 2010, working closely with the office of then-Prime Minister Stephen Harper and the RCMP, which was coordinating security with U.S. Homeland Security and U.S. intelligence. On the ground were 21,000 security personnel.
The police terrorized the protesters, with many Toronto police removing their badges so that they could not be identified. More than 1,140 people, including many bystanders, were arrested. Mounted police, along with others on foot, charged the demonstrators with batons and injured countless people. Hundreds of people were "kettled" and kept, without cause, for hours in the pouring rain to suppress the people's affirmation of their rights.
2. Marco Mendicino is a former federal prosecutor who was prosecution co-lead in the case of the so-called "Toronto 18" in which a group of national minority youth were "entrapped" by the Canadian state which used two CSIS moles who were paid handsomely for their work. At the end, seven of the youth had their charges dropped because there was no case against them. They were not compensated for their mistreatment and did not receive an apology from the police or the government and will forever bear the burden of being a "terror suspect." Others "confessed" under blackmail to being involved in terrorist activity. They were told they would serve long prison sentences if they were to resist.
(With files from TML Weekly, Global News, U.S. Department of State Archive, PMO.)
Canada's Subservient Defence Policy
Billions Spent on Military Procurement

On August 4, the Department of National Defence (DND) announced the beginning of production for 360 Armoured Combat Support Vehicles (ACSV) at the General Dynamic Land Systems (GDLS) production facilities in London, Ontario. GDLS is a subsidiary of General Dynamics USA, the fifth largest weapons manufacturer in the U.S. The contract is valued at $2 billion. According to DND, "This fleet can be used in a wide variety of roles, such as part of Canada's contribution to NATO's assurance and deterrence measures in Central and Eastern Europe, or in the Canadian Armed Forces' response to natural disasters in Canada."
 This announcement
followed another from DND on July 31 on the delivery of the first of
six Arctic and Offshore Patrol Ships (AOPS) for the Canadian Navy, the
HMCS Harry DeWolf, built by the Irving Shipyards in
Halifax. DND notes: "Specifically designed to patrol Canada's offshore
waters and northernmost regions, this new class of ship will be at the
core of an enhanced Canadian Armed Forces (CAF) Arctic presence,
effectively complementing the capabilities of our other current and
future warships through critical reconnaissance and surveillance
activities. In addition to highly versatile platforms that will enable
the ship to support a variety of domestic and international missions."
This announcement
followed another from DND on July 31 on the delivery of the first of
six Arctic and Offshore Patrol Ships (AOPS) for the Canadian Navy, the
HMCS Harry DeWolf, built by the Irving Shipyards in
Halifax. DND notes: "Specifically designed to patrol Canada's offshore
waters and northernmost regions, this new class of ship will be at the
core of an enhanced Canadian Armed Forces (CAF) Arctic presence,
effectively complementing the capabilities of our other current and
future warships through critical reconnaissance and surveillance
activities. In addition to highly versatile platforms that will enable
the ship to support a variety of domestic and international missions."
Apart from the six AOPS, Irving is building two coast guard vessels. Together they make up the first part of the "Combat Package" that was awarded to Irving under the National Shipbuilding Strategy (NSS) which was announced by the former Harper Conservatives and now made operational and expanded under the Trudeau Liberals who have shown themselves to be even greater warmongers than the Harperites. The initial cost of $38 billion for the NSS has almost doubled to $70 billion to date and will likely increase to many more billions.
Additionally, Canada is poised to purchase 88 new jet fighters from one of three armaments monopolies, at a cost of $19 billion, which is being opposed in a national campaign led by Canadian Voice of Women for Peace and their allies.
All of the tens of billions being spent on boosting of military hardware is being justified in the name of Canada's defence policy under the Liberals -- "Strong, Secure, Engaged" -- adopted in 2018, which aims, among other things, to increase "significant and strategic long-term investments that will ensure the Canadian Armed Forces continues to function as an agile, and combat-ready force, capable of making tangible contributions and delivering on its commitments at home and around the world." The Liberals committed $62.3 billion over the next 20 years to boost Canada's military under their new policy. In an effort to divert the anti-war movement in Canada, these large amounts of money being handed over in pay-the-rich schemes to Irving Shipbuilding Inc., GDLS and others are being justified in the name of job creation and boosting the economy! Under the so-called Industrial and Regional Benefits (IRB) Policy, introduced in 2014, companies that are awarded "military procurement contracts must undertake business activity in Canada equal to the value of the contract."
 Even as Canadians
are in the midst of dealing with the coronavirus pandemic which is far
from over, the Liberals are quietly pushing through their military
procurement. In this they have the support of the other cartel parties
in the Parliament, all of whom are on side with Canada's foreign policy
based on modern day colonialism, imperialism and war under the dictate
of U.S. imperialism and its instruments NATO and NORAD. This is the
essence of the "Strong, Secure, Engaged" foreign policy.
Even as Canadians
are in the midst of dealing with the coronavirus pandemic which is far
from over, the Liberals are quietly pushing through their military
procurement. In this they have the support of the other cartel parties
in the Parliament, all of whom are on side with Canada's foreign policy
based on modern day colonialism, imperialism and war under the dictate
of U.S. imperialism and its instruments NATO and NORAD. This is the
essence of the "Strong, Secure, Engaged" foreign policy.
This increased drive to militarism and war by the Trudeau Liberals and the other cartel parties must be stopped by the stepped-up organized resistance of the Canadian people to U.S. imperialism, NATO and NORAD. It is the Canadian people who must decide on Canada's military policy, foreign policy and the future of Canadian society. It is they who must step up their organizing for an anti-war government and work to make Canada a zone for peace. In this way Canadians can make a decisive contribution to peace in the Americas and the world, and contribute to securing a permanent peace in the world which is the condition for the flourishing of all peoples and nations.
All Out to Make Canada A
Zone For Peace!
Organize for an Anti-War Government!
(With files from Government of Canada, Department of National Defence. Photos: TML)
First Anniversary of Revocation of Jammu and Kashmir's Special Status
Oppose Indian Government's Brutal Suppression of the Kashmiri People! Long Live Their Struggle for Freedom, Justice and Democracy!

Demonstration, August 2019, in Lahore, Pakistan against India's brutal
occupation of Kashmir.
August 5, 2020, marked the first anniversary of the revocation of Jammu and Kashmir's special status under Article 370 of the Indian constitution. After abruptly changing the semi-autonomous nature of India-controlled Kashmir, the Indian government imposed a media lock-down and curfew and started brutally arresting, imprisoning and killing Kashmiris from all walks of life. The Indian government used the Armed Forces Special Powers Act it adopted in 1990, giving itself license to arrest, search and destroy property, and kill with impunity.
The Kashmiri people resisted this latest crime against their homeland and their people and have continued fighting back courageously for the past year, uncowed by the brutal attacks against them. The crimes against the people of Kashmir have been met with the solidarity of the people of neighbouring Punjab who too have long experience of the impunity of the Indian armed forces. India's actions have come up against widespread condemnation from peoples all over the world.
In Kashmir, prior to the first anniversary, authorities imposed a curfew on the city of Srinagar on August 3 with immediate effect until the anniversary itself, marked as a "Black Day" by the people.

Demonstration held at the British Parliament marking the first
anniversary of the revocation of Jammu and Kashmir's special status.
Projected on the side of the building is
"Kashmiri Lives Matter."
On August 5, to oppose the Indian government's suppression and lock-down which amount to a siege of Jammu and Kashmir, demonstrations were held in India, Britain and other places. In Britain a mass action was held outside the Indian High Commission in London, and the Council House in Birmingham, a city where 150,000 Kashmiris live. Hundreds of Kashmiris participated in these two significant actions.
 The Kashmiri people themselves
have been asserting their right to self-determination for many decades,
dating back to the partition of India in 1947, in which the British
state played a nefarious role to perpetuate its colonial rule over the
sub-continent using forms of government based on preserving
Anglo-American values and representatives. An important demand in the
present situation is that the people of Jammu and Kashmir must be
allowed to settle the Kashmir issue through a fair, transparent and
democratic referendum under the auspices of the United Nations, as
required by UN resolutions.
The Kashmiri people themselves
have been asserting their right to self-determination for many decades,
dating back to the partition of India in 1947, in which the British
state played a nefarious role to perpetuate its colonial rule over the
sub-continent using forms of government based on preserving
Anglo-American values and representatives. An important demand in the
present situation is that the people of Jammu and Kashmir must be
allowed to settle the Kashmir issue through a fair, transparent and
democratic referendum under the auspices of the United Nations, as
required by UN resolutions.
Large numbers of Indian troops have been used to suppress the movement of the people of Kashmir for independence. The leadership of the movement has been incarcerated, and new psychological methods of disorientation and oppression are being applied. There have been a massive number of arrests in Kashmir, along with the violence of the Indian military against the people. The Sino-Indian confrontation has also added to the already fraught situation in Kashmir.
Further, thousands of Indian workers are being brought to Jammu and Kashmir for work and settlement by the Indian government, demonstrating Indian Prime Minister Narendra Modi's hurry to obliterate the identity and heritage of Kashmir. It is reported they brought with them many of the more than 19,000 cases of COVID-19 recorded in Kashmir.
The peace- and justice-loving people of Canada stand with the people of Kashmir in their struggle for self-determination. May their march for freedom, justice and democracy win victory!
(Photos: WW, S. Omer)
Filipino People's Struggle for Democratic Rights and National Liberation
Duterte's State of Union Address Condemned
at Home and Abroad

Action in Toronto on eve of President Duterte's State of the
Nation Address, July 27, 2020.
Militant actions were held in the Philippines, in Canada and elsewhere on the eve of U.S.-backed Philippine President Rodrigo Duterte's State of the Nation Address (SONA) on July 27. The Communist Party of Canada (Marxist-Leninist) stands as one with Canadians of Filipino origin and their allies against the Duterte regime's campaign of state terror, violence and impunity against the people. A state of martial law exists in the Philippines, aimed at crushing the national liberation movement of the Filipino people led by the Communist Party of the Philippines (CPP).
In its message to the tens of thousands of demonstrators in the Philippines who courageously defied the government's ban on public gatherings to oppose Duterte's disinformation, the CPP saluted the determination and resolve of the people. By demonstrating in public in their numbers, CPP wrote, the people express their "widespread and intense indignation against the regime's incompetence, corruption, fascism and repressive measures, complete disregard and abandonment of the people's well-being."
To mark the occasion, Bayan Canada, the alliance of progressive Filipino organizations, held public actions in Vancouver, Winnipeg, Toronto, Ottawa and Montreal, and an online rally in Calgary and Edmonton. These actions brought together youth of Philippine heritage and their peers, migrant workers, and friends and allies including activists of CPC(M-L).

Ottawa, July 27, 2020.
Filipino youth in particular stood tall and spoke out against the crimes of the government of President Duterte including the extra-judicial killings of some 30,000 people in the name of the "War on Drugs." Speaker after speaker condemned the Duterte regime for its refusal to assist the Filipino people during the coronavirus pandemic and, instead, its use of the crisis to step up the "counter-insurgency" campaign against the revolutionary movement, carrying out political assassinations and other acts of repression. Duterte's recently passed Anti-Terrorism Act, 2020 was soundly condemned as a draconian law which seeks to enhance government police powers.
The Filipino people are determined to win victory,
to strengthen and advance their revolutionary movement, to oppose U.S.
and other big power domination of their country, and to advance the
cause of peace and justice. Bayan Canada Secretary General Rhea Gamanna
noted on the day of action that the Filipino people have a long
anti-imperialist tradition and a fighting history and that, by relying
on their own efforts and broad political unity, they will oust the
U.S.-supported Duterte regime.

Winnipeg, July 27, 2020.
(Photos: Bayan Canada)
CPC(M-L)'s Message to the People's State of the Nation Address Action to Hold the Rodrigo Duterte Regime to Account

Action in Vancouver on eve of President Duterte's State of the Nation
Address, July 27, 2020.
The Communist Party of Canada (Marxist-Leninist)
brings you warm greetings to this SONA ng Bayan, the People's State of
the Nation Address action to hold the Rodrigo Duterte regime to account
for the escalating state violence and terror being committed with
impunity against the Filipino people. We condemn the so-called Anti-Terrorism Act 2020
and express our confidence in your actions to stop it.
Our Party also expresses its sincere condolences on the loss on July 23 of Fidel V. Agcaoili, esteemed Chairperson of the Negotiating Panel of the National Democratic Front of the Philippines. Comrade Agcaoili's important role in negotiations with the Philippines government to find a peaceful but just resolution to the more than 60-year civil war in the Philippines provides important guides to action for those who take his place.
Please also accept our deepest sympathies for the losses you have suffered this year as a result of state repression and crimes committed against your comrades. We hail their courage and heroism and send their comrades and families our condolences and support.
Close to 30,000 people have died as a result of extrajudicial killings and political assassinations. Thousands of people have been imprisoned for providing support to the people in the form of medicines and food during the COVID pandemic.


Montreal, July 27, 2020.
With the passing of the so-called Anti-Terrorism Act 2020 this month the Duterte government reveals its desperation and that of its U.S. backers to crush the people's resistance led by the CPP and NPA. The so-called Anti-Terrorism Act 2020 also expresses the interests of the U.S. to ensure the Philippines remains a stable military base for asserting its presence in Asia and to challenge China. It is part of U.S. imperialist war preparations which the people do not condone.
The joint military naval and other exercises the U.S. conducts with the Philippines and their "counter-insurgency" exercises must be ended as the CPP and the NPA are leading the people to achieve. The anti-communist hysteria of the ruling circles in the Philippines is a reflection of the strength of the Filipino people's movement for national liberation and the desperation of the enemy.
Duterte also continues to hand over the Philippine economy to powerful foreign interests, increasing economic displacement, poverty and migration. Tens of thousands of people are forced by circumstances to leave the islands in search of relief abroad.
Canada is itself an architect of unacceptable practices which encourage human trafficking and abuse of women and children and migrant workers. The Canadian government also champions the theft of the Filipino people's mineral wealth and lands by mining companies and others pursuing narrow private interests, committing crimes against the people to quell their resistance.
Canada's silence about the crimes committed against the people is unacceptable. Silence is violence.
Our Party works to realize the just demand that all migrant workers in Canada be granted permanent residency and receive all public supports as a matter of right.
Workers of Filipino origin are an integral part of the Canadian working class. We work as one for peace, freedom and democracy.
Glory to the Life and Work
of Comrade Fidel Agcaoili!
Long Live the Resistance of the Filipino People!
Long Live Our Unity in Action! The People Will Prevail!
No to Fascist Violence and Terror by the U.S.-supported Duterte Regime!
No to the So-called Anti-Terrorism Act 2020!
(Photos: Bayan Canada, Gabriela)
|

The Communist Party of the Philippines (CPP) with profound sorrow informs that Comrade Fidel V. Agcaoili, Chair of the Negotiating Panel of the National Democratic Front of the Philippines, passed away suddenly in Utrecht, Netherlands of a pulmonary arterial rupture. Comrade Agcaoili served as a member of the NDPF from the early 1990s and as Chair since 2016 in efforts to achieve a just and permanent peace in the struggle between the Filipino people led by the CPP and the U.S.-sponsored Philippine state.
The CPP states:
"Filipino communists and revolutionaries feel a deep sense of sorrow and loss with Ka (Elder) Fidel's passing. He was one of the most beloved and respected leaders of the Party, the National Democratic Front of the Philippines (NDFP) and the Filipino people. Over the past decades, from the underground movement, to inside prison, to international work and peace negotiations, Ka Fidel untiringly struggled with the Filipino people and served the revolutionary movement and all the oppressed and exploited classes to achieve national and social liberation. At all times, Ka Fidel firmly upheld the principles of the Party. He was imbued with the communist spirit to his last breath."
The death of Comrade Fidel V. Agcaoili is a great loss to the CPP, the NDFP and the entire Filipino people. The Communist Party of Canada (Marxist-Leninist) sends it deepest condolences to his comrades, his family and all the Filipino people in the homeland and in Canada, in particular our comrades in Bayan Canada, Migrante, Philippine Solidarity Group, Gabriela and other fighting organizations.
May the life and work of Comrade Fidel V. Agcaoili serve to inspire our joint efforts for our collective rights, justice and peace and strengthen fraternal relations between the people of Canada and the Philippines.
Honduras
Kidnapping of Indigenous Leaders:
Black Garífuna Lives Matter!

Protest in Triunfo de la Cruz against kidnapping of Garífuna
activists, July 26, 2020.
The Garífunas are a community of black Indigenous people who have lived on the north coast of Honduras since 1797, when they fled the island of Saint Vincent and the Grenadines after the defeat of their insurrection against the British Empire. Although recognized by the Honduran government in the late 19th century, the territory claimed by the Garífuna has been the object of intense disputes since the early 20th century.
In the beginning, it was the transnational banana companies that put strong pressure on the Garífuna territory. At that time, the Honduran state was one of the main agents of the transnationals, violating the ancestral right of the Garífuna people over their territory and granting authorization for the cultivation of thousands of hectares of banana plantations. Today, once again with the complicity of the Honduran government, it is the cultivation of the palm tree -- an African palm widely used by the cosmetic industry -- that exerts strong pressure on this territory. It is estimated that 80 per cent of the Garífuna territory is occupied by the cultivation of the African palm, while at the same time, the Honduran government has stimulated occupation of the Caribbean coast by the high standard tourism industry with the construction of resorts on Garífuna lands.
 At the end of the
70s, more precisely in 1978, with the creation of OFRANEH (Black
Fraternal Organization of Honduras), the fight began to preserve what
was left of the territory occupied by the Garífuna for more
than 200 years. There are 48 Garífuna communities spread
along the Caribbean coast of Honduras, with an economy based on family
farming.
At the end of the
70s, more precisely in 1978, with the creation of OFRANEH (Black
Fraternal Organization of Honduras), the fight began to preserve what
was left of the territory occupied by the Garífuna for more
than 200 years. There are 48 Garífuna communities spread
along the Caribbean coast of Honduras, with an economy based on family
farming.
It is important to remember that in 2009 Manuel Zelaya, the democratically elected president, was overthrown in a coup d'état orchestrated by the military and financed by the large companies operating in the country. One of the most important aspects of the Zelaya government's policy was precisely to check the interests of foreign agribusiness in Honduras and the latifundios (large estates). So now, once again, the Honduran state is serving the powerful against the interests of the communities.
In this context, four Garífuna social activists were kidnapped (Alberto Sneider Centeno, Milton Joel Martínez Álvarez, Suami Aparicio Mejía and Alber Sentana Thomas), from the community of Triunfo de la Cruz, in the municipality of Pantalla. The kidnapped activists are linked to the fight for land, the preservation of the environment and respect for human rights. Alberto Centeno led the efforts to make the Honduran state comply with the decision issued by the Inter-American Commission on Human Rights in 2015 and with Convention No. 169 of the International Labour Organization which deals with consulting Indigenous peoples over the occupation of their territories. The kidnapping was carried out on July 18 by a heavily armed group wearing the uniforms of the Honduran security forces.
 It is important
to bear in mind that the Honduran people are mobilizing themselves to
ensure that the four are returned alive and well.
It is important
to bear in mind that the Honduran people are mobilizing themselves to
ensure that the four are returned alive and well.
We demand:
- that the Honduran government rescue the four kidnapped activists and that they be returned alive to the Garífuna people;
- the immediate compliance with ILO Convention No. 169;
The Communist Party of Canada (Marxist-Leninist) calls on Canadians to demand the Government of Canada take a principled position against the gross violations of human rights carried out by the coup government of Honduras which they supported when it came to power and started committing atrocities.
The kidnapped Garífuna activists must be returned to their families and communities. These abuses of human rights and appropriation of Garífuna territory must stop.
(With files from Resumen Latinoamericano, August 3, 2020. Translated from original Spanish by TML. Photos: Ofrenah)
The Fight of Revolutionary Cuba for Its Right to Be
Helms-Burton Lawsuit Dismissal Sets Precedent

Picket against the U.S. blockade of Cuba, Montreal, July 17, 2020.
In the United States, federal judge James Lawrence King has dismissed a lawsuit, under Title III of the Helms-Burton Act, against the cruise ship company Carnival for use of property in Cuba.
Javier Garcia-Bengochea, a Cuban-American in Florida, holds a certified stake in the port at Santiago de Cuba used by the cruise ship. The property was confiscated by the Cuban government in 1960 following the Revolution. Garcia-Bengochea inherited the property in 2000.
As part of its increased hostilities against Cuba, the Trump administration ended the suspension of Title III of the Helms-Burton Act in May of 2019. Title III allows U.S. nationals with alleged claims to properties confiscated by the Cuban government to seek compensation from companies operating on those properties, however the Act states that for "property confiscated before March 12, 1996, a United States national may not bring an action under this section on a claim to the confiscated property unless such national acquires ownership of the claim before March 12, 1996."
The decision is key for claims under the Helms-Burton
Act, as it sets a precedent for the immediate future.
Carnival faces a similar lawsuit for the use of facilities in the port
of Havana, still pending a decision by federal judge Beth Bloom in a
Miami court. Some 6,000 claims on property confiscated by the Cuban
government are estimated at a value of $2 billion, or as high as $8
billion with interest.
(With files from Miami Herald.)
Cuban Sappers in White Lab Coats

Cuban medical team arrives in Surinam, March 20, 2020, to assist in
combatting COVID-19.
It is always said that sappers risk their lives to save the lives of thousands of people when they clear minefields in conflict situations.
In pandemic times, such as the one humanity is suffering today with COVID-19, it is the doctors and health workers who take on this dangerous work for the benefit of millions of citizens around the world.
The members of Cuba's famous peaceful army of white lab coats are currently true sappers, because they go to the most complex corners of planet Earth to fight the deadly disease face to face.
They do so in Africa, Europe, and Latin America and the Caribbean, defying the risks they face in the line of fire on the front line of the battle against COVID-19.
Their only goal is to defeat death, and they accomplish it with conviction, humanism and great altruism, legacies left to them by the historical leader of the Cuban Revolution, Fidel Castro, and the Moncada generation, the one that on July 26, 1953 took up the struggle for the island's true independence.
There is no doubt that the members of the Cuban Medical Brigades who serve in many countries around the world are genuine heirs of those young people who, led by Fidel, assaulted the Moncada Barracks 67 years ago, the heroic deed that led to the triumph of the Revolution on January 1, 1959.
On the Day of National Rebellion in the Caribbean nation, this July 26, the sappers in white lab coats deserve special recognition. Far from their homeland and their families, they defeated the pandemic and gave another lesson in dignity and courage.
Through their example, they have also defused the campaigns to discredit Cuban medical collaboration, orchestrated by the United States, and at the same time they have further hoisted the flags of solidarity with Cuba and against the increased blockade that Washington imposes on the island.
Today, from all regions of the world, there are calls for Cuba’s doctors and health workers to be awarded the Nobel Peace Prize for the humanitarian work they have done over many years.
And of course the Cuban sappers in white lab coats deserve that laurel and many more, but they already have the most valuable one, the recognition of the peoples and the millions of people whom they have cured and brought back to life.
(Cubadebate, July 27, 2020. Translated from original Spanish by TML. Photo: J. Vidal)
Spanish Journalist Gives Colombian Foreign Minister Fitting Reply
Edgar Eddie Ferreira is a Spanish journalist who stopped Colombian Foreign Minister Claudia Blum in her tracks after she declared not long ago that "Cuba is an extremely poor country whose backwardness is evident in its infrastructure."
- Yesterday, 200 million children slept in the streets because they are homeless, and I assure you none of them are Cuban, but many are Colombian.
- Millions of people in the world have no medical coverage and I assure you that none of them are Cuban. In Colombia alone more than half the population is without medical insurance and those who do have it are not attended to in a 100 per cent efficient manner.
- In the world there are millions of illiterate people and none of them are Cuban, but many are Colombian.
- So far this year, social leaders have been assassinated all over the world, but none in Cuban territory. In Colombia, they are killed on a daily basis and the president does nothing to stop this state massacre of the people.
- In culture, sports, health and education Cuba is the best in the region. The day Colombia is able to surpass Cuba in any kind of social progress, you can offer your opinion. In the meantime, look at your own country and think how great an island like Cuba is compared to Colombia, which in spite of having all the natural resources to be a great country, does not come across in the world today as anything good because it is considered the most corrupt, the most murderous, the most drug-trafficking, the most ignorant, it has the highest unemployment rate in the region, the highest murder rate, and your president is a travelling circus, spewing lies and stupidities wherever he goes.
- Foreign Minister, my friend, I am telling you all this because I am a Spanish journalist and I have had the opportunity to travel to Cuba, just like I got to know and have worked in Colombia. Living and working in Colombia is a real challenge for a journalist, who can be killed at any time for practicing their profession; last year alone in Colombia 36 journalists were murdered. In Cuba, no one is murdered for thinking differently. If Cuba is poor, Colombia is a misery compared to Cuba.
(Resumen Latinoamericano, July 31, 2020. Translated from original Spanish by TML.)
On the Passing of Eusebio Leal, Historian of the City of Havana
The Sweet and Consoling Union of Love and
Hope for the Homeland

On July 31, the Cuban nation was saddened to learn of the passing of Dr. Eusebio Leal Spengler, the renowned and much loved City of Havana Historian. Eusebio Leal led a life of service, dedicated to preserving the authentic historical and cultural patrimony of Cuba and its people. He did this through his teachings and writings and, notably, through his vital work to preserve and restore the beautiful heart of historic Havana -- Havana Vieja.
Eusebio Leal was a member of the Central Committee of the Communist Party of Cuba and an elected deputy of the National Assembly of People's Power of Cuba. TML Weekly is publishing below a tribute to his life and work written by the editorial staff of Radio Havana.


How difficult a blank page is at this moment. There are no words that can fill the emptiness or describe the sadness and shock that Cubans who loved and admired him felt on receiving the news.
There were years of intense work, rescuing our patrimony, returning a part of our identity to those of us who were born on the Island. We never imagined how much effort there was behind each undertaking, how many years of sacrifice, of incessant struggle. Eusebio Leal Spengler dedicated his life to that.
His physical disappearance pains us, has shocked us. We thought he was immortal, a man who would always be here to preserve not only Old Havana but the entire Cuban patrimony which he loved so much. But once again death has played a trick on us.
 "We are part of
the great challenges and great moments," this great man would say at
times. He was not only part of them; he was a witness, a maker of
ideas, of dreams, of realities, he battled against windmills, but
achieved results. He was a Quixote of our time.
"We are part of
the great challenges and great moments," this great man would say at
times. He was not only part of them; he was a witness, a maker of
ideas, of dreams, of realities, he battled against windmills, but
achieved results. He was a Quixote of our time.
In 1981, by decision of the Government, the Office of the Historian of the City of Havana took up the great challenge of carrying out the first restoration plan. Behind that enormous effort, after so many years of pushing for it, was Leal. And he carried it successfully for decades, nourishing a dream-reality, returning the capital to its splendour, nurturing the spirituality of every human being, little by little transforming our perception of a city that has already seen five centuries of existence.
As he himself said, a work like this, with international impact and public recognition, could only be accomplished in a Revolution like ours, with the support of a leader like Fidel. And our Historian had to live through an intense and fruitful time that began for him in 1959, when the process of revolutionary changes, of renovation in all areas of Cuban society began. This idea is what reaffirms his deep revolutionary conviction: "We are the custodians, the inheritors and continuers of the cultural, social and political heritage of a nation."
Hero of Labour of the Republic of Cuba, a Cuban who has received countless awards, decorations and honourary doctorates, Leal has been, thanks to his "gladiatorial stewardship," the discoverer and re-discoverer, every day and for years, of his Havana, our Havana. From a very young age, he dreamed of restoration, something he accomplished in spades. He was fortunate to have Emilio Roig de Leuchsenring, the first City of Havana Historian, as his teacher and guide, whose vitality and love for the capital he imbibed, to the point of declaring: "Without Emilio Roig there would be no Eusebio Leal."
A lover of books, a Christian, a militant patriot, a total son of his times, Leal is, as Dr. Ana Cairo once said, a great example of revolutionary humanism in Cuba, because he polemicized, he accessed new knowledge, he shared his knowledge, listened to people and was moved by their spiritual needs.
We further quote Dr. Cairo who, with her typical clairvoyance said: "Leal is an example of the best virtues, a representative of a generation that was self-taught, but whose humble origins did not lead to his marginalization, two things that today seem to go together. In his case it showed that one can be poor and have education, civility and culture [...]. Leal must continue to be a model for Cuban society."
In everything that Leal did, in everything he defended, we cannot forget his patriotic vision, grounded in the ideas of Marti -- "that sweet and consoling union of love and hope for the homeland" -- thanks to which he carried out truly invaluable transformations for the country.
 In this sense,
Eduardo Torres-Cuevas, another one of our most profound intellectuals,
once asserted -- also repeating a phrase from Martí: "I
believe that Leal was truly one of the most real and valuable men of
our time ... Understanding reality and working to change what had to be
changed of that reality, and at the same time [understanding] the
utility of the work, the utility of virtue. And that demanded of him --
which was natural -- a professional and human ethic that imbued all of
his work. It would be difficult for me to try and speak in a fragmented
way about Leal's work. One way or another, his work extended over a
wide field, and I would say that this breadth was a result of the
utility of his vision, of a non-pragmatic utility, of what had to be
done and how to do it, how to produce really useful transformations. We
are talking about a utility that mainly relates to values."
In this sense,
Eduardo Torres-Cuevas, another one of our most profound intellectuals,
once asserted -- also repeating a phrase from Martí: "I
believe that Leal was truly one of the most real and valuable men of
our time ... Understanding reality and working to change what had to be
changed of that reality, and at the same time [understanding] the
utility of the work, the utility of virtue. And that demanded of him --
which was natural -- a professional and human ethic that imbued all of
his work. It would be difficult for me to try and speak in a fragmented
way about Leal's work. One way or another, his work extended over a
wide field, and I would say that this breadth was a result of the
utility of his vision, of a non-pragmatic utility, of what had to be
done and how to do it, how to produce really useful transformations. We
are talking about a utility that mainly relates to values."
At the Book Fair that was dedicated to Leal, the Historian of the City of Havana stated that he wished life was longer to give him the opportunity to do more and more, because what he had done so far seemed meagre to him. But by way of an anecdote he concluded that all was not in vain. He put it this way: "A few days ago, as I was walking through a plaza in Old Havana, a father approached me with his little son so the boy could greet me. I asked him: And what do you want to be when you grow up? And the boy replied: Me? A historian.
"That is why Eusebio Leal has kept his spirits up and always gets re-energized. Previous historians did it, Doctor Roig did it. I have had to do it, others will have to do it. They will appear with other names [...]. What we have sown and what we have done, he concluded, we must hope and have faith that it will bear fruit in the new generations."
(Radio Havana, August 1,
2020. Translated from original Spanish by TML. Photos: Radio Havana)
|
|

COVID-19 Update
World Health Organization Directives on
Preventing COVID-19 Transmission
As Canada begins to emerge from strict lockdown measures and enters a phase of loosening the restrictions which served to flatten (though not yet reverse) the infection curve, international experience and the advice of the World Health Organization (WHO) hold importance for us going forward.
In his July 13 coronavirus situation briefing, the Director General of WHO characterized, in broad strokes, four stages of the pandemic and said what "we're seeing is countries that overcame the first peak of the outbreak, but having eased restrictions, are now struggling with new peaks and accelerating cases. In several countries across the world, we are now seeing dangerous increases in cases, and hospital wards filling up again. It would appear that many countries are losing gains made as proven measures to reduce risk are not implemented or followed."
WHO has set out recommendations, including measures to keep COVID 19 transmission in check. Its recommendations contained in its Scientific Brief entitled "Transmission of SARS-CoV-2: implications for infection prevention precautions" dated July 9 are based on a detailed review of dozens of recent scientific studies of how COVID-19 infection is transmitted.
"Based on what we currently know, transmission of COVID-19 is primarily occurring from people when they have symptoms, and can also occur just before they develop symptoms, when they are in close proximity to others for prolonged periods of time. While someone who never develops symptoms can also pass the virus to others, it is still not clear to what extent this occurs and more research is needed in this area."[1]
The July 9 report outlines transmission factors in detail and from the scientific evidence to date reached definite conclusions which resulted in the formation of the following recommendations on how to keep COVID 19 transmission in check:
- Identify suspect cases as quickly as possible, test, and isolate all cases (infected people) in appropriate facilities;
- Identify and quarantine all close contacts of infected people and test those who develop symptoms so that they can be isolated if they are infected and require care;
- Use fabric masks in specific situations, for example, in public places where there is community transmission and where other prevention measures, such as physical distancing, are not possible;
- Use of contact and droplet precautions by health workers caring for suspected and confirmed COVID-19 patients, and use by health care workers of airborne precautions when aerosol generating procedures are performed;
- Continuous use of a medical mask by health workers and caregivers working in all clinical areas, during all routine activities throughout the entire shift;
- At all times, practice frequent hand hygiene, physical distancing from others when possible, and respiratory etiquette; avoid crowded places, close-contact settings and confined and enclosed spaces with poor ventilation; wear fabric masks when in closed, overcrowded spaces to protect others; and ensure good environmental ventilation in all closed settings and appropriate environmental cleaning and disinfection.[2]
On July 13 the Director General concluded his briefing with these words: "I want to be straight with you: there will be no return to the "old normal" for the foreseeable future. But there is a roadmap to a situation where we can control the disease and get on with our lives. But this is going to require three things:
"First, a focus on reducing mortality and suppressing transmission.
"Second, an empowered, engaged community that takes individual behaviour measures in the interest of each other.
"And third, we need strong government leadership and coordination of comprehensive strategies that are communicated clearly and consistently.
"It can be done. It must be done. I have said it before and I will keep saying it."
Working people do not have control over what measures are taken by governing authorities but they are speaking out -- front line health care workers, transit workers, teachers and education workers, miners and industrial workers, retail, hospitality and child care workers, migrant workers in farm and meat packing industries and many more.
TML Weekly and Workers' Forum report on the experiences of workers who have organized when employers refused to do it, which now includes contact tracing; of mine workers in Quebec whose union played a key role in determining health and safety measures for return to work underground; of transit workers speaking out for mandatory use of masks on mass transit; of teachers speaking out for government to implement safe working conditions for reopening of schools; of migrant workers demanding status as key to achieving safe working and living conditions. It is the working people taking up social responsibility and advocating for constructive measures they know will protect themselves and society at large that is the decisive element as we go forward.
Notes
1. WHO Director General Briefing, July 13, 2020.
2. "Transmission of SARS-CoV-2: implications for infection prevention precautions, WHO, July 9, 2020.
Six Months into the Pandemic
The end of July marks six months since the World Health Organization (WHO) declared a Public Health Emergency of International Concern on January 30, and nearly five months since the WHO declared the situation a global pandemic on March 11.
Unfortunately, the spread of the virus is not under control. In these six months, the million mark for reported cases of COVID-19 was reached on April 2. The 2-million mark was reached 13 days later on April 15. Roughly another million cases were recorded in each 12-13 day period until the end of May, when a million new cases were added in only nine days. Compare that to the end of July, where a million new cases were reported in four days alone, between July 26 and 30.
At this time, many countries have moved into some stage of reopening their economy, where lock-down and physical distancing measures are being lifted. In this situation, the coronavirus pandemic overall continues to worsen because not all countries are implementing the kinds of measures necessary to prevent contagion. The situation is better where such measures are implemented. As of July 31 the figures provided by Worldometers are:
- Total reported cases: 17,540,901
- Total active cases: 5,871,057
- Closed cases: 11,669,844
- Deaths: 677,924
- Recovered: 10,991,920
The daily rate of new cases has been increasing since mid-May, when it briefly plateaued at about 100,000 new cases per day. Since then, the rate has increased to as high as 289,609 on July 24.
The rate of daily deaths has also increased since reaching a low in late May, when daily deaths ranged from 3,123 to 5,379, to late July when daily deaths ranged from 4,190 to 7,179. Reporting of deaths follows a seven-day cycle from low to high, due to when data is collected and submitted.
The rate of recoveries is also increasing which is good news. This is attributed to broader shared experience around the world of how COVID-19 infections manifest and which treatments are effective. The bad news is that ongoing research is revealing long-term effects for those who overcome the infection, such as serious damage to major organs.
But it is too early to draw systematic conclusions of any kind. On May 12, the WHO provided guidance on reopening, saying that a basic condition to be met is a rate of positive tests of five per cent or lower for at least 14 days, as well as having capacity in the health care system to manage further outbreaks, and to ensure that timely testing and contact tracing can be carried out immediately to stem any new outbreaks. These guidelines on reopening remain the reference point as the pandemic situation improves in some countries and worsens or resurges in others.
Regarding the various vaccines being developed around the world, Canada's Chief Public Health Officer Dr. Theresa Tam stated at an August 4 press conference that COVID-19 and its containment will be a serious public health issue for years to come.
"We're planning, as a public health community, that we're going to have to manage this pandemic, certainly over the next year, but planning for the longer term, over the next two to three years, during which the vaccine may play a role. But we don't know yet," Tam told reporters.
Deputy Chief Public Health Officer Dr. Howard Njoo noted that "People might think that if we get a vaccine then everything goes back to normal the way it was before. That's not the case... All of the measures we've put in place now will still have to continue with the new reality for quite some time." He added that "Certainly I think that we need to temper people's expectations, thinking that the vaccines can be that silver bullet that will take care of everything, and everything we've done up to now won't be necessary in the future."
Tam said that while an effective vaccine would be a "very important aspect of the response," it shouldn't be seen as a way to end the pandemic. She warned that even once a vaccine is tested and deemed to be both safe and effective, "It's likely that there won't be enough vaccines for the population. So there'll be prioritization and we're looking at that."
Tam said public health officials are planning for a scenario in which measures that have been put in place thus far, including physical distancing and limiting crowd sizes, could be required even after a vaccine is found.
"[A vaccine] is one important layer of protection," said Tam. "It is a very important solution if we get a safe and effective vaccine, but I would say that the public health measures that we have in place -- the sort of personal, daily measures that we take -- are going to have to continue."
This update provides information on Canada as well as the United States, Mexico, Brazil, South Africa and India where the highest number of COVID-19 infections and deaths have been recorded.
Canada
In Canada, the number of reported cases during the
course of July rose from 104,271 to 116,312. Daily new cases have
ranged from 67 to 786. The number of active cases has declined from
27,912 to 6,150. Deaths rose from 8,615 to 8,935. Daily deaths ranged
from 2 to 26. Nationally, the rate of positive tests is 2.6 per cent.
Rates of infection and death are down considerably since their peak in
early May.
The 118,187 cases in Canada as of August 5 are distributed by province
as follows:

At this stage, all provinces and territories are at some stage of reopening.
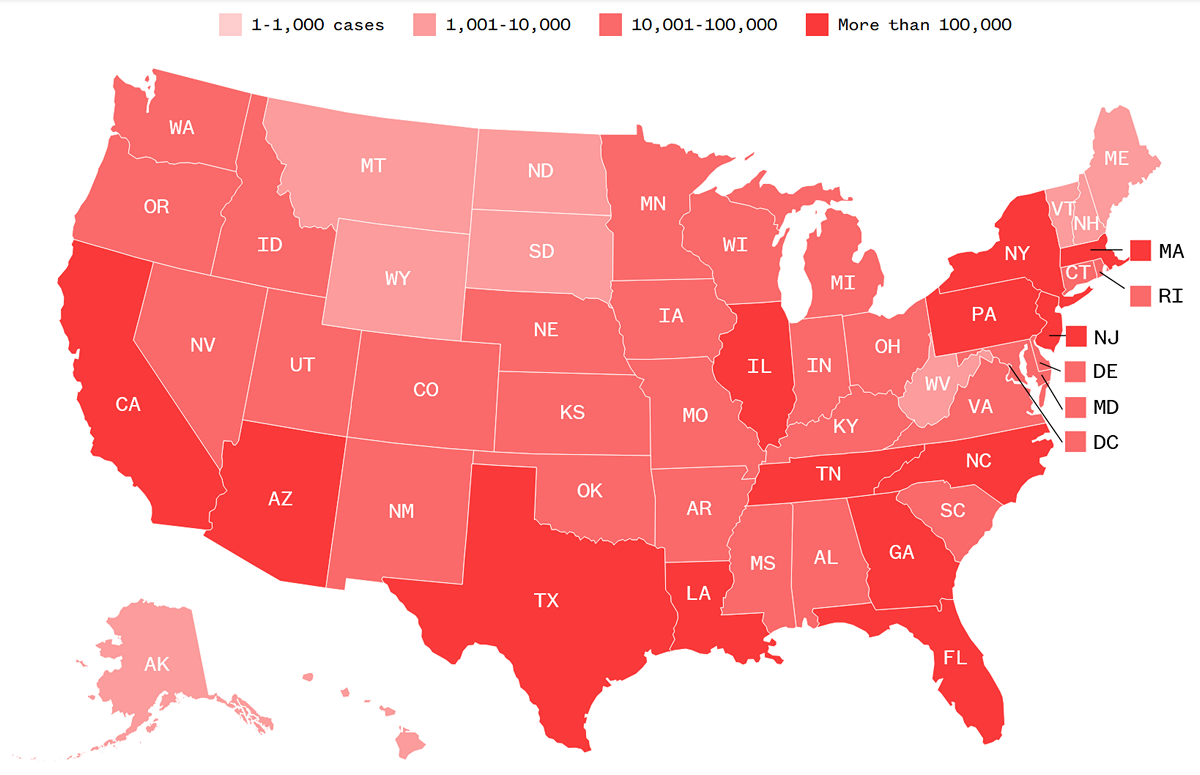
United States
As of the end of July, the U.S. continued to lead the world as the country with the highest total number of infections and deaths. New cases of COVID-19 have started to decline. On August 2 and 3, the U.S. recorded fewer than 50,000 new cases per day. In July, the average was 60,000 new cases per day. That said, by August 7, the U.S. will have exceeded five million reported cases. On a per capita basis, the U.S. has amongst the highest rate of infection as well, exceeded only by small countries or principalities, most with populations of four million or less. In terms of death rate, the U.S. ranks 10th in the world, after several European countries as well as Chile and Peru.
To put things further into perspective, while the U.S. accounts for less than five per cent of the global population, it has 22 per cent of the world's global coronavirus deaths and more than 25 per cent of the recorded infections. As of August 4, its positivity rate (the percentage of people who test positive) is 20.9 per cent.
Various states continue to push ahead with reopening and lifting of physical distancing and other safety measures despite not having the situation under control, because policies are not being set based on looking after the people's well-being. As of August 6, there are 37 states with a higher than recommended rate of positivity, ranging from just over 5 per cent to 22 per cent. Of these 37 states, 18 have reopened or are reopening, eight have paused reopening and 10 are reversing their reopenings.
Mexico
In Mexico over the course of July, the total number of COVID-19 cases rose from 226,089 to 416,179. Daily new cases ranged from 4,482 to 8,438 in July. On July 31, Mexico moved into third place in the number of fatalities, behind the United States and Brazil, with 46,688 deaths. Mexico also moved into sixth place globally in the total number of confirmed cases, where it remains in early August. Mexico implemented lockdown measures on March 24, and began a phased reopening of the economy on May 18, beginning with municipalities that had zero confirmed cases of COVID-19 and are not adjacent to municipalities where there were confirmed cases. From May 18 to the end of the month, preparations for broader reopening were made, with attention paid to sectors of the economy deemed to be essential: manufacturing of transport equipment, mining and construction. On June 1, a traffic light system was implemented -- green, yellow, orange and red -- representing the severity of the pandemic in each state, updated weekly, to indicate which activities are safe to resume.
As concerns the positivity rate, on July 1, Mexico's rate was 50 per cent, five times higher than the WHO guideline to safely reopen. Furthermore, Mexico is carrying out a very limited number of tests -- as of August 6 it has conducted 1,041,860 tests. This puts it at number 41 among all countries and territories; on a per capita basis its testing rate puts it at 150th in the world. News agencies report that Mexico's policy is to test only the sickest of patients. Deputy Health Minister Hugo Lopez Gatell, an epidemiologist, said in late May that anything more would be "a waste of time, effort and resources," and that "Our purpose is not to count every case, but to use modern and efficient mechanisms to tackle the pandemic." More recently in July, Lopez Gatell said, "deaths in our country are associated with diabetes, hypertension and obesity."
All of this indicates community transmission is running very high, that the number of infections is greatly under-reported, especially since those who are infected but not severely ill are unknowingly transmitting the disease. Lopez Gatell's remarks suggest that contact tracing is also likely not being practiced in any systematic way.
An important factor that is exacerbating the pandemic is the condition of Mexico's health care system. While Mexicans ostensibly have universal health care, in practice the system does not provide them with adequate care. During the pandemic, the situation has gotten worse. The government of President Andres Manuel López Obrador (AMLO) has been implementing an austerity program since coming to office, that includes cuts to the health care system that was already not in good shape. The New York Times reported in late May that "In Mexico, it's not just the coronavirus that is claiming lives. The country's broken health system is killing people as well.
"Years of neglect had already hobbled Mexico's health care system, leaving it dangerously short of doctors, nurses and equipment to fight a virus that has overwhelmed far richer nations.
"Now, the pandemic is making matters much worse, sickening more than 11,000 Mexican health workers -- one of the highest rates in the world -- and depleting the already thin ranks in hospitals. Some hospitals have lost half their staff to illness and absenteeism. Others are running low on basic equipment, like heart monitors.
"The shortages have had devastating consequences for patients, according to interviews with health workers across the country. Several doctors and nurses recounted dozens of preventable deaths in hospitals -- the result of neglect or mistakes that never should have happened."
Brazil
During the course of July, the number of reported cases in Brazil rose from 1,453,369 to 2,666,298. Since early June, Brazil has had the second highest number of COVID-19 cases in the world. The number of daily new cases in July ranged from 48,458 to 70,869. The total number of deaths rose from 60,713 to 92,568 during July. The number of cases per capita is also very high, as is the number of deaths per capita, comparable to the U.S. As of August 6, the positivity rate in Brazil is 31.76 per cent.
Already the situation in May was known to be serious and getting worse. Nonetheless, Brazilian states began the process of reopening in early June despite indications that the conditions to do so safely did not exist.
Raquel Stucchi, a professor at the Campinas State University (Unicamp) School of Medicine, and member of the Brazilian Infectious Disease Society (SBI), explained the situation in a July 10 article published in Brasil de Fato. She warned "that with the expansion of the reopening of commerce, restaurants, bars, gyms and beauty parlors, starting this week in the state capital, it is probable that there will be a rise in contagion due not only to exposure in the workplace, but also on public transport.
"The expert explains that neither São Paulo nor any other place in the country, has seen enough of a decline in transmissions that would justify the resumption of commercial activities, like happened in Europe.
"'No country has behaved like Brazil. These cities are reopening, or at least being more flexible, before we have seen a flattening of the curve. What's going to happen is that we will learn sooner or later in many parts of the country, that we will be forced to have two weeks of openings, two weeks of closures, two more of openings, two more of closings, this is the Brazilian way,' she highlights."
On July 9, Brasil de Fato quoted a former Health Minister in the government of Dilma Rousseff, who explained the political basis for the pandemic and the push by social movements in Brazil to remove Bolsonaro from office:
"This tone that minimizes the disease, is the strategy adopted by the president since the arrival of the novel coronavirus in Brazil. Denial, according to physician and former Health Minister Alexandre Padilha, is part of a political effort to ensure the economy doesn't crash amid the tragedy.
"'Bolsonaro is motivated by genocidal logic -- he has made that clear -- he believes this pandemic will only be over when 70 -- 80 per cent of the population has been infected, and that this should happen as quick as possible, so as to not get in the way of restarting the economy.' says Padilha, who is now a Federal Congressman.
"For the parliamentarian, the deaths caused by the coronavirus are already the biggest human tragedy in Brazilian history, for two fundamental reasons: the negation of science by the president of the Republic and the weakening of the public health care system (SUS). Padilha says that the only solution is to remove Bolsonaro from power.
"'I'm one of those who believe that Brazil won't be able to stop this genocidal project and will not be able to recover economically under Bolsonaro's leadership. The impeachment requests and the efforts to impede this government are fundamental in order for Brazil to avoid, along the years, the deepening of the human tragedy we are living due to COVID-19,' suggests the former minister."
Regarding the situation facing health care workers in the country, Brasil de Fato reported on July 29 that "On the frontlines of the battle against COVID-19, 325 nurses, technicians and nurse assistants have lost their lives working in Brazil's health care system. The data was published by the Nursing Observatory, an arm of the Federal Nurses Council (COFEN), created to evaluate the impact the pandemic is having on professionals in the sector.
"Brazil alone accounts for 30 per cent of the deaths of nurses on the planet. The international organization that unites national nursing councils under one umbrella, the International Council of Nurses (ICN), confirms the numbers. The entity's political advisor, Hoi Shan Fokeladeh says that, 'with the last update of the numbers in June, we know that Brazil had the highest number of nurse deaths.'
"Out of the total, 64 per cent of victims are women, who in large part were practicing their professions. The largest number of deaths, 35.4 per cent, occurred in the country's southeast, where the states of São Paulo, Rio de Janeiro and Minas Gerais are located.
"The northeastern and northern regions, which have poorer populations and more precarious health care infrastructure, account for 27.2 per cent and 21.5 per cent respectively.
"In Brazil, where there is an average of 2.4 nursing professional deaths every 24 hours, the Nursing Observatory shared that almost 30,000 nurses, technicians and assistants have contracted COVID-19."
South Africa
South Africa has been experiencing a sharp rise in COVID-19 cases since June. In July, the number of reported cases rose from 159,333 to 493,183. The number of daily new cases ranged from 8,124 to 13,944 and have been declining since then. Deaths from COVID-19 rose from 2,749 to 8,005 during July. As of August 4, South Africa's positivity rate was 16.9 per cent.
On July 24 Associated Press reported that "Global hot spot South Africa is seeing a 'huge discrepancy' between confirmed COVID-19 deaths and an unusually high number of excess deaths from natural causes, while Africa's top health official said Thursday [July 23] the coronavirus is spreading there 'like wildfire.'" The AP report continues:
"A new report by the South African Medical Research Council, released late Wednesday [July 22], shows more than 17,000 excess deaths from May 6 to July 14 as compared to data from the past two years, while confirmed COVID-19 deaths have surpassed 6,000.
"'The numbers have shown a relentless increase -- by the second week of July, there were 59 per cent more deaths from natural causes than would have been expected,' the report says.
"The council's president, Glenda Gray, said the excess deaths could be attributed to COVID-19 as well as other widespread diseases such as HIV and tuberculosis while many health resources are redirected toward the pandemic.
"Meanwhile, some South Africans are thought to be avoiding health facilities as fears of the new virus spread and public hospitals are overwhelmed.
"'The coronavirus storm has indeed arrived,' President Cyril Ramaphosa told the nation Thursday evening as cases surpassed 400,000. He announced that schools would 'take a break' for a month to protect students.
"South Africa now has the world's fifth largest caseload. It makes up more than half the confirmed cases on the African continent with 408,052.
"One of the country's nurses was buried Thursday, the latest of more than 5,000 infected health workers across South Africa.
"Duduzile Margaret Mbonane died just a month before her retirement, her husband said. [...] 'The government must assist our nurses with protective clothing,' said Duduzile's husband, Herbert Mbonane. 'Maybe my wife wouldn't have died if personal protective equipment were made available in time.'
"Those on the front lines have been hit hard: The World Health Organization said Thursday more than 10,000 health workers have been infected in its African region, which is largely sub-Saharan Africa."
Regarding the situation of Africa as a whole, the WHO Regional Office for Africa reported on July 30 that:
"COVID-19 infections in Africa will exceed one million cases in the coming days as the pandemic surges in several hotspot countries. In a little more than three weeks, the number of cases on the continent almost doubled to 889,457, with 18,806 deaths.
"Overall, the pandemic is accelerating with the number of new cases increasing by 50 per cent during the last 14 days compared with the previous fortnight. However, only five countries account for about 75 per cent of the cumulative COVID-19 cases -- they are Algeria, Egypt, Ghana, Nigeria and South Africa. South Africa alone accounts for around half of the continent's total cases. Deaths are also increasing. A total of 4,376 new deaths were recorded during the last 14 days, representing a 22 per cent increase from the previous two weeks.
"Seven countries in sub-Saharan Africa which had imposed lockdowns and have now started easing them have experienced a 20 per cent jump in cases over the past two weeks. Some countries such as the Republic of the Congo and Morocco have had to re-implement partial restrictions because of an increase in cases."
"As Africa approaches one million cases, the continent is at a pivotal point," said Dr Matshidiso Moeti, World Health Organization (WHO) Regional Director for Africa. "The virus has spilled out of major cities and spread into distant hinterlands. Countries need to keep apace and urgently decentralize their key response services. We can still stop COVID-19 from reaching full momentum, but the time to act is now."
The WHO Africa adds that one of the "most important collective responsibilities is to protect frontline health workers, who are at high risk. Forty-one African countries have reported nearly 14,000 health worker infections. In 16 countries which reported health worker infections over the past month, nearly a quarter recorded an increase in the past two weeks compared with the preceding fortnight.
"Expanding the scale and quality of public health measures such as testing, contact tracing, isolation and care of patients remain central to the response, as well as preventing infection through handwashing, physical distancing and wearing of masks. Lifting of lockdowns that have helped to slow down the spread of COVID-19 should be evidence-based, phased and targeted.
"As borders start to re-open and with the Islamic holiday, Eid al-Adha, about to begin on [July 31] marked by social and religious gatherings, there is a concern that the virus could spread further, even to areas that are still untouched by COVID-19, if necessary precautions are not taken. [...]
"WHO recently released guidance to countries and communities on public health measures for Eid Al Adha in the context of COVID-19.
"Under-reporting of cases is a challenge as testing for COVID-19 in Africa remains low by global benchmarks, but capacity has expanded significantly. About 7.7 million tests have been performed since February. The number of tests performed per 10,000 population as of mid-July was below 100 in 43 countries out of the 54 assessed. This must improve.
"Although infections are on the rise across the continent, the trend is varied. Nine countries in sub-Saharan Africa have reported a decline in cases over the past three weeks. Gabon and Mauritania have made significant progress, with the time it takes for case numbers to double increasing. In Djibouti and Tunisia, very few cases have been reported for the last few weeks, and most are imported. In Egypt, Africa's second-most populous country and one of the hardest hit by COVID-19, a decline in cases has been observed over the last five weeks.
"WHO is supporting countries' response to COVID-19 by providing technical guidance, crucial medical equipment and has remotely trained more than 72 000 health workers and partnered with regional and national professional associations to build on existing capacity. Through an online supply portal, WHO, other United Nations agencies and partners have also organized shipments of more than 650 requests of key equipment, including more than 2,400 oxygen concentrators to 47 countries in the region."
India
During the course of July, the total number of reported COVID-19 cases in India rose from 605,220 to 1,697,054. Daily new cases ranged from 19,428 to 57,704, and the rate of new infections appears to be increasing. Total deaths in July rose from 17,848 to 36,551, with the number of daily deaths ranging from 438 to 783, and continuing to rise into August. The positivity rate is 8.9 per cent as of August 4. As of August 7, India has 2,033,847 cases, the third highest number in the world.
India began lifting national lockdown measures in late May, based on considerations that were not founded on sound epidemiological considerations nor the people's well-being. As the pandemic has continued and worsened in India, the actions of the government of Prime Minister Narendra Modi have made clear that its objectives regarding the pandemic are not directed at upholding the well-being of the Indian people.
In a July 29 op-ed for the Guardian, Jayati Ghosh, a professor of economics at Jawaharlal Nehru university, New Delhi, summed up the experience of the Modi government's handling of the pandemic:
"The central government's approach to public health has been miserly, incompetent and insensitive. Containment policies copied from China and Europe display no recognition of the lived reality of much of India's population. Social -- more accurately physical -- distancing can't be done by people in crowded and congested homes with five or more people living in one room. Frequent hand-washing is a luxury when access to clean water is limited, and it must be collected through lengthy, arduous journeys made by women and girls. But officialdom has seen no need to adjust these guidelines or make it possible for poor people to achieve them. And treatment for the infected varies hugely according to income: public hospitals are overcrowded and overstretched; private ones charge stratospheric rates.
"The official attitude to the estimated 100 million or more rural-urban migrants who build India's towns and cities and provide their services was even more telling. Early into the lockdown, special repatriation flights were arranged for Indians stranded abroad. But internal migrants got no such relief for two months; they were deprived of their right to livelihood but only -- and rarely -- received the most paltry compensation. When, in desperation, they travelled on handcarts, containers and cement mixers or simply walked hundreds of kilometres to get home, they faced beatings, detention, being sprayed with disinfectant, even being killed on rail tracks where they slept thinking that no trains were allowed. The arbitrary dusk-to-dawn nationwide curfews (with no public health rationale) forced them to walk in the blazing heat. When special train services for such migrants were finally started, nearly two months into lockdown, impoverished workers had to congregate in stations in large numbers to get tickets, expose themselves to infection and then pay full fares. Conditions on these trains were often so appalling, with delayed journeys in intense heat without food and water provision, that in just 10 days in May, 80 people died on board.
"India's public distribution system, which currently holds nearly 100 million tonnes of food grain stocks, could have been used to feed the newly hungry. But only small amounts have been released for free distribution even as evidence of starvation grows, and this parsimony has been compounded by the obscenity of selling some food stocks to convert into ethanol for making hand sanitisers. Meanwhile, the single-minded focus on COVID-19 means that other health concerns of the poor are ignored or given less attention. Tuberculosis has been the biggest killer of the poor in India, but many TB patients have not received treatment. Immunization of children has suffered and hospital births have fallen by 40 per cent."
Recent reports indicate questionable activity on the part of Prime Minister Modi surrounding the Prime Minister's Citizen Assistance and Relief in Emergency Situations Fund (the PM Cares Fund). The day after it was set up on March 27, Modi appealed to "all Indians" to donate. The need for a new fund has been publicly questioned when the similar PM National Relief Fund (PMNRF) has existed since 1948.
The BBC reported on June 30:
"On the day PM Cares was set up, a massive humanitarian crisis began to unfold in India -- millions of migrant workers, some of India's poorest people, began fleeing the cities after Mr Modi imposed a sudden country-wide lockdown. For weeks, they walked hundreds of miles, hungry and thirsty, to reach their villages. More than 100 died. [...]
"In the weeks since the fund was set up, questions have also been asked about how it is constituted and managed, how much money has been collected, from whom, and how it is being put to use?"
The PM Cares fund has refused to disclose its operations to the public. A July 14 report from the Associated Press says that the agency "requested a list of donors and payments from Modi's office under the Right to Information Law, which gives citizens access to information from India's often opaque bureaucracy. The request was denied.
"Modi's office, which manages PM CARES, has refused to disclose the information, arguing that even though it is administered by the Indian government, it is not a public authority, and therefore not subject to right-to-information laws. As a result, there is little transparency about the money the fund is receiving and spending in the middle of India's still-raging virus outbreak. [...]
"Modi is the fund's chairman, and the powerful home minister, Amit Shah, and the ministers of defense and finance sit on its board. But unlike other government-administered funds, it isn't audited by India's Comptroller and Auditor General. Instead, Modi appointed a private business consulting firm, SARC & Associates, to audit the fund 12 days after it donated $212,665 to it.
"Sunil Kumar Gupta, the head of SARC & Associates, has been a vocal supporter of Modi's Bharatiya Janata Party, appearing in photographs with Modi and top party leaders at various events."
The value of the fund is now speculated to be well over $1 billion. Despite this vast amount, AP reports that only $13 million was given to state governments to assist the millions of migrant workers stranded without work or transportation home during the two-month countrywide lockdown, to provide food, shelter, medical treatment and transportation.
As well, community health workers who are having to bear the brunt of education and prevention work are being denied proper remuneration and the conditions to safely do their work. AP reported on August 7 that "About 900,000 members of an all-female community health workforce began a two-day strike Friday [August 7], protesting that they were being roped in to help with contact tracing, personal hygiene drives and in quarantine centers, but were not being given personal protective equipment or additional pay, according to organizer A.R. Sindhu.
"The health workers, known as Accredited Social Health Activists, or ASHA, which means 'hope' in several Indian languages, have been deployed in each village on behalf of the Health Ministry. Their work includes escorting children to immunization clinics and counseling women on childbirth.
"While their regular work hasn't been reduced, they are increasingly being involved by state governments in the fight against the pandemic, said Sindhu. 'ASHA workers don't have masks or PPEs or even sanitizers,' she said.
"She added that, although the work has increased
and become more dangerous, their salaries remain static at roughly $27
per month. And the families of at least a dozen women who she said died
from COVID-19 didn't receive compensation from India's federal
insurance for front-line health care workers because their causes of
death were not recorded as COVID-19."
|
(To access articles individually click on the black headline.)
Website: www.cpcml.ca Email: editor@cpcml.ca